The National Association of State Emergency Medical Services (EMS) Officials has just released the Pediatric Transport Products for Ground Ambulances, Version 2.
The document is a resource for EMS providers to determine existing options for securing infants and children who are transported by ambulance.
Over 1 million pediatric patients are transported by ambulances nationwide each year. There are an estimated 5,000 ambulance-involved crashes annually, with 10% involving infants or children.
The Centers for Disease Control and Prevention (CDC) has noted that ambulances are 2.5 times more likely to be involved in a crash than an automobile. While ambulances are generally well equipped to secure adult patients, many are lacking proper devices to secure their youngest patients whose varying sizes make the challenge even greater.
A recent study found that of 200 ambulances observed carrying 206 pediatric patients, more than half of the patients were lying on the stretcher, and 11% were unrestrained. Additionally, 27% of observed pediatric patients were unrestrained on the bench seat, 10% were on the lap of a parent or EMS provider, and 13 different types of medical equipment were minimally secured or not secured at all.
Why is there such a diversity of ways that infants are transported in ambulances? There are multiple factors, including:
Lack of Standards Increases Risk
There are no established guidelines for infant patient transport, only recommended best practices. This puts each EMS organization and ambulance provider in the position of deciding how they will handle infant patient transport.
Insufficient Funding
Up to now, the preferred method of infant patient transport required both a transport incubator and a dedicated ambulance that could accommodate it.
A transport incubator can cost between $50,000 and $80,000, while an ambulance to carry it could cost $300,000 or more. Many EMS organizations and ambulance providers cannot fund this level of investment.
Risk to the Infant Transport Crew
One factor that is widely overlooked is that a transport incubator during an ambulance accident can break free and injure or kill the infant transport crew. Some ambulance providers refuse to transport infant patients for fear of liability issues.
Separating the Child from the Mother
Many ambulances are designed to carry one patient. If the cot is being used to transport the infant, the mother may have to be transported in another ambulance. This not only ties up two ambulances- mothers sometimes refuse to leave the child during transport.
Infant Transport is Time Consuming
When infant patient transport using an incubator is required, the process disrupts the normal operations of both the ambulance provider and the involved hospital staff.
Typically, the ambulance crew must go to the location where the travel incubator is stored. They may have to remove seating and storage from the vehicle. They then must load and secure the incubator, which may weigh 250 pounds or more. They drive to the sending hospital, unload the incubator, and take it to the pediatric unit.
The hospital team prepares the infant for transport and loads the child in the incubator. The transport team then loads and secures the incubator and drives to the receiving hospital. The unload the incubator, take it to the pediatric unit, and the hospital team unloads the child.
The ambulance crew then must load the incubator, drive it to the storage facility, unload it, and reinstall the seats and storage.
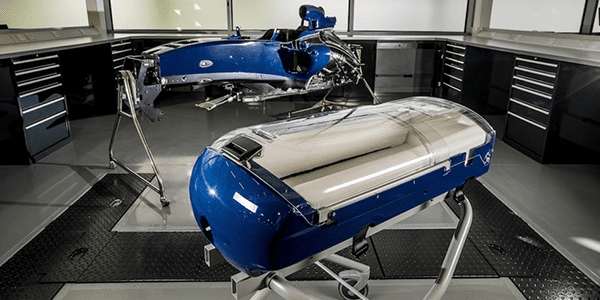
The Baby Pod 20 – Born from Tragedy
After a series of deadly infant transport accidents, an engineer became obsessed with solving the problem.
While watching a Formula 1® race one day, he saw a car hit the barriers at over 200 miles per hour. Seeing the driver walk away from a crash that destroyed the car around him, he realized there was a better way;
Replace the heavy incubator with a smaller, lighter, infant transport device. Less weight equals less mass, less inertia, and less danger to the patient and ambulance crew.
He approached one of the world’s leading manufacturers of Formula 1® racing cars. They quickly saw the need for a safer infant transport device and put their expertise, time, and talent to work.
Thus, the Baby Pod was born.
The Baby Pod 20 is safer, more affordable, and more efficient than travel incubators.
The Baby Pod 20 was designed to overcome all the disadvantages of a transport incubator.
SAFER
The Baby Pod 20 is designed and built with the same materials as a Formula 1® racing car. Altogether, there are four distinct layers of protection for the child:
- The outer shell of Baby Pod 20 is constructed of carbon fiber, which is a strong, yet lightweight and durable material. It acts as a rigid cocoon to protect the infant from flying debris.
- The Baby Pod 20’s internal shock absorbent foam is constructed of polyurethane foam with a PUNL® removeable cover, which remains breathable, yet is impervious to liquids and solutions. The foam interior surrounds the infant’s head, feet, and sides during transport and is designed to help protect the infant in the event of impact.
- The vacuum mattress is manufactured from a soft foil and is filled with flame-retardant polystyrene beads. Removal of the air from the vacuum mattress via the attached valve allows secure positioning of the baby within the Baby Pod 20. It also reduces discomfort caused by road vibration as well as dampens traffic noise.
- Maintaining the infant’s core body temperature during transport is critical. That is why up to now, transport incubators were necessary. The Baby Pod 20 incorporates the Transwarmer™ Infant Transport Mattress which is designed to provide radiant heat and additional shock absorption to the infant during transport. Unlike an incubator, the Transwarmer™ Infant Transport Mattress does not require electricity to maintain the infant’s core temperature.
In addition to these four layers of protection, the Baby Pod 20 incorporates additional state of the art safety innovations to protect the infant. With all these features the Baby Pod 20 can withstand 20Gs of force in four directions and up to 10Gs vertically or inverted making it the safest infant transport device available.
MORE AFFORDABLE
A typical transport incubator costs around $60,000 and requires a dedicated vehicle that can cost up to $360,000. You can buy seven Baby Pod 20 Infant Transport Devices for the cost of one incubator.
MORE EFFICIENT
Typical time to transport an infant using an incubator in a dedicated incubator ambulance is between 7 and 8 hours. Typical time to transport an infant using a Baby Pod 20 in any ambulance or aircraft is 3 to 4 hours.
With all these advantages over travel incubators, it is easy to see why EMS organizations, ambulance providers and hospitals are beginning to adopt the Baby Pod 20 as their primary infant patient transport device.
NASEMSO plans comprehensive crash testing
NASEMSO created the Pediatric Transport Products for Ground Ambulances resource to minimize the confusion by allowing the EMS industry to compare the products available.
Inclusion of a product in the Pediatric Transport Products for Ground Ambulances resource does not imply that it has been deemed “safe” or is endorsed by NASEMSO. Unfortunately, there are no minimum safety criteria to be included in the product list, because such criteria have not been developed.
Unlike child carseats used in automobiles, which must meet rigorous safety standards developed by the U.S. Department of Transportation, there are no such requirements for child transport devices used in ambulances. Further, industry experts agree the testing criteria for child seats designed for automobiles do not apply to the patient compartment of an ambulance.
NASEMSO hopes to fill this gap by organizing and leading a comprehensive crash testing project to determine pass/fail criteria for these pediatric transport products. The project will be a collaborative effort involving national EMS organizations, manufacturers of the equipment (who will donate their devices for the crash testing research), safety engineers, and pediatric experts. The crash testing research is expected to be a five-year effort before the criteria are developed and standards are published. In the interim, NASEMSO urges EMS providers to utilize devices specifically designed for child transport in ambulances.
View the Pediatric Transport Products for Ground Ambulances, V2.